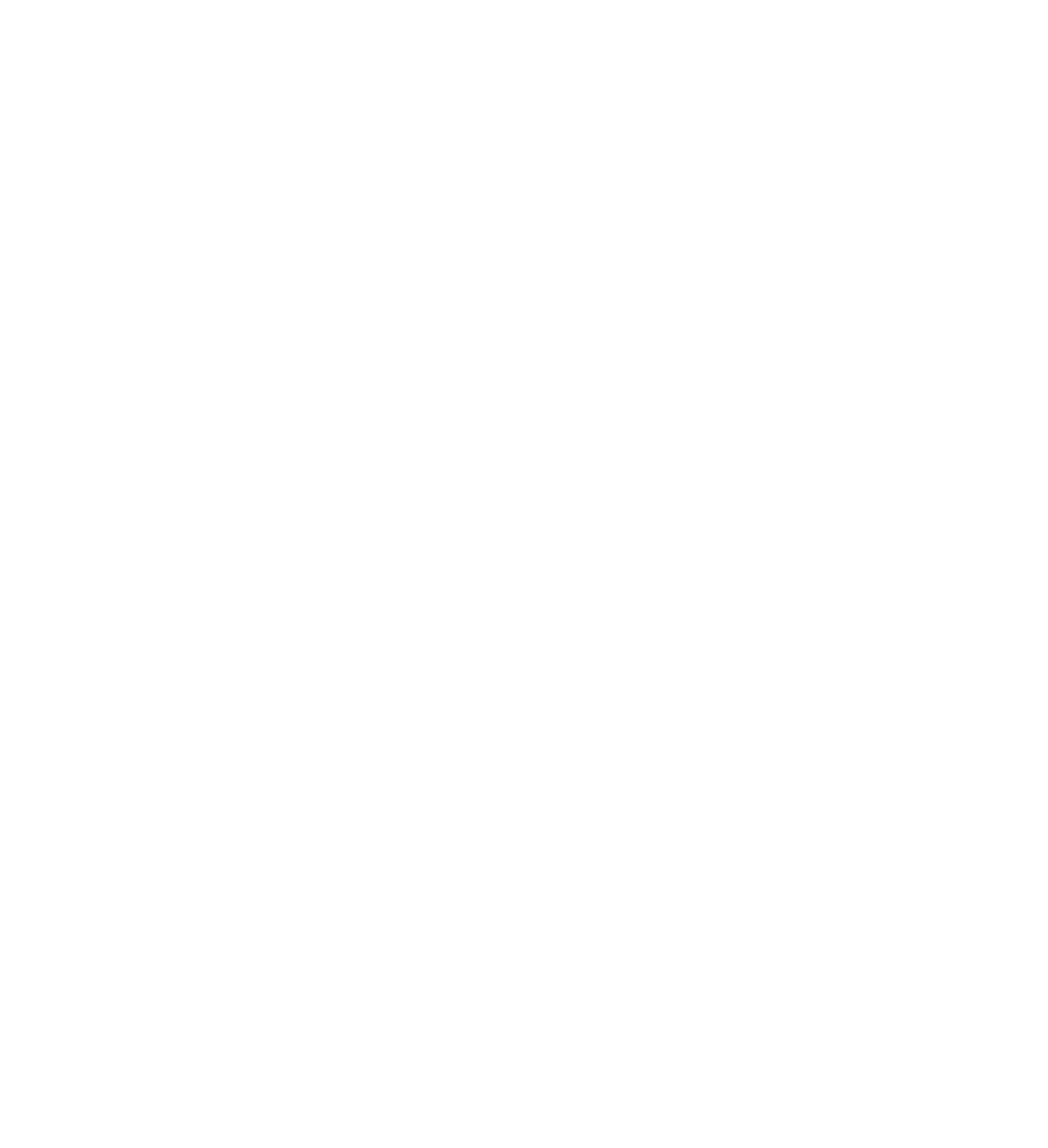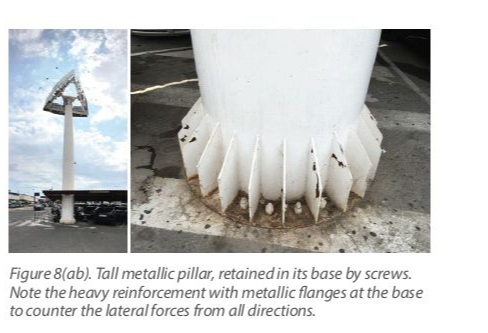
Although the screw can consistently withstand axial forces, its capacity is drastically reduced when it comes to lateral forces causing bending of the screw. To counter this, tall metal pillars held by screws will not only have many screws in their base, but also reinforce it with supporting flanges to counter lateral forces (Figure 8). The bending due to lateral forces increases the risk of both unscrewing and fatigue fractures. Other factors can reduce the load-bearing capacity of the screws and increase the risk of plastic deformation and fracture. A common such factor is the reduction of friction by a lubricant such as plaque or saliva (Figure 9). The presence of plaque and saliva in the screw channel (28) will lower friction and increase the clamping force produced under the same torque, leading to unintentional “overtightening.” This could bring the screw closer to the plastic deformation threshold, which might lead to a fracture under the functional load. When a reconstruction loosens, plaque can very quickly migrate into the screw channel with a lubricating effect. If the screw were to be tightened without prior cleaning, the friction will be drastically reduced, resulting in increased preload, risking future unscrewing or fracture.
Another critical factor is a misfit between the different components of the screw joint. This could result in a skewed or adverse force applied on the screw and consistently uneven elastic elongation, drastically reducing the capacity of the screw to serve under functional load. Screw loosening is one of the most frequently encountered problems in general, encountered in Sweden by about 10% of the patients within 5 years (29).
Complications Manifested in the VeneerVeneering complications, either as fractures, cracks, or “chipping,” are common in implant-supported FDPs. Although there is a significant diversity in the prevalence depending on the material and extent of the prosthesis, in general in Sweden, approximately 14% of patients experience such problems within 5 years (29). Although such complications at first appear due to functional forces and loading, the truth is that very often some compromise in the design predisposes to such complications by lowering the tolerance of the prosthesis to damaging forces. For example, veneering porcelain which is not properly supported by the metal framework will crack easier under “normal” functional forces (Figure 10).
Another often neglected “predisposing” risk is the misfit of components, which has been shown to also lead to cracks and chipping of the veneering. Ceramic materials are hard and brittle and are easily weakened by cracks. Veneering porcelain has a much lower elastic modulus than metals and, although it can bear a heavy load, it is very sensitive to any “bending” forces. Discrepancies and gaps of up to 500 µm could evade clinical assessment, as the prosthesis could still be placed with torque tightening of the screws (30). If a multi-unit bridge is tightened in the presence of even minor misfit, it will be subjected to a certain amount of “bending,” leading to tension being formed. Such tension is tolerated very differently by the metal framework than by the lower elasticity ceramics. Although not leading to immediate problems, studies have shown that even minor misfits of 150 µm can significantly increase the frequency of veneer chipping under functional load (Figure 31).
Complications Manifested in the Abutment and the Implant
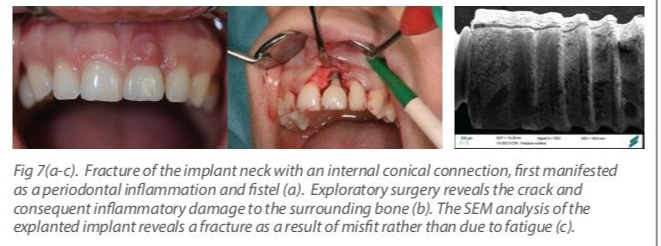
Fractures of the titanium abutment or the implants are rare and encountered in general below 0.5% of cases (29). A common underlying reason is misfit, which can result in high stress concentrated on a small part of the abutment or implant neck (Figure 10), resulting in acute plastic deformation or fracture.
Summing up complications and overloading
The damaging effects of excessive or adverse loading can be manifested on the peri-implant bone and tissue or on the mechanical implant components. It is difficult to clinically quantify the magnitude and direction of naturally occurring occlusal forces, which makes an exact definition of excessive forces or "overload" elusive at present. At the same time, the alveolar bone has a significant ability to adapt to functional load, while its tolerance varies among individuals, location, and other anatomic and physiological parameters. Total loss of osseointegration due to excessive or adverse loading appears possible with an already osseointegrated dental implant, but this has been very rarely documented. Bone density and the quality of bone are large influencing factors.
The components of the implant-abutment-prosthesis complex are designed to function under heavy load and are tested in vitro to withstand challenging functional conditions. Nevertheless, in clinical reality, we can encounter complications due to excessive or adverse load, often manifested in the abutment and prosthesis screws, the veneering, and less frequently the implant and the abutment bodies. However, certain design factors can drastically reduce the capacity of the implants to withstand functional loading and predispose them to complications by amplifying the effects of forces. Such factors are typically related to improper design, subjecting the implants to adverse lateral forces (Figure 11) and/or misfit (Figures 10, 13) between the different components.