The principle of CMA is to establish Class I Molars and Canines relationship by activation of the appliance with heavy inter-arches force I, 2 elastics (1/4 “ 6 oz and 3/16” 8 oz,). Class II elastics with anchorage provided by the clear retainer or fix appliance at the opposite arch. Full-time wear of Class II elastics (22 hours daily) is required. It is also recommended to change elastics every 4 hourly. Phase I treatment usually takes 6–8 months to complete. The patient compliance and co-operation must be high, and alignment of both arches must be combined with uses of clear aligners or fixed appliances after 6-8 months. (1)
CASE REPORT 1
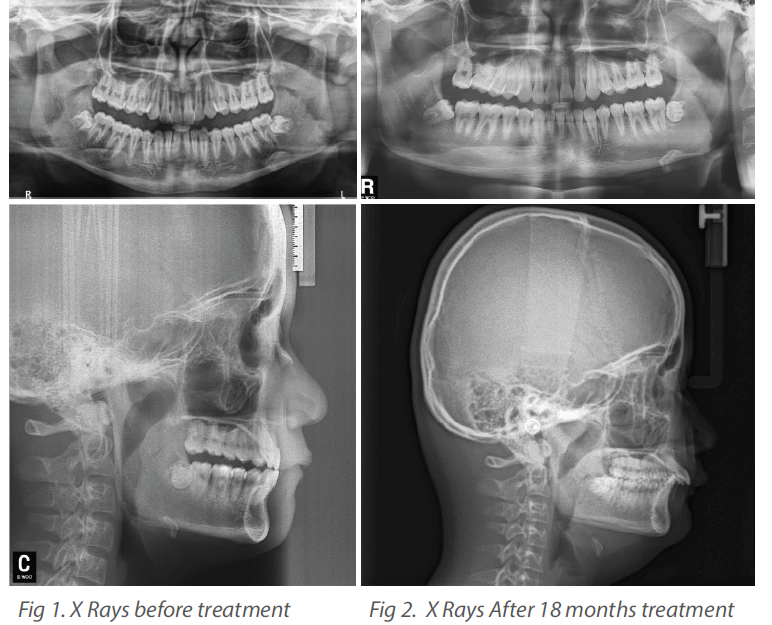
Young boy aged 13yr 8m were referred by other dentist to prescribe Mandibular Advancement (MA) protocol by Invisalign. The overbite were 100% deep and lower incisors were traumatizing the upper soft tissue. The over jet was 10mm with lower face retruded and short. Previous patient seen an orthodontist, who had suggested to use Herbst appliance but were declined by patient. From the lateral x-ray we could expect significant amount of adolescent growth since there is concavities developing at the lower border of C2 and C3, the lower border of C4 is flat and C3 and C4 are more rectangular in shapes. Aligners with Mandibular Advancement Function design were worn for 10 months without many improvements and the Carriere Motion 3D appliance were prescribed using full day 6 oz 1/4” Class II elastics bilaterally together with vibration accelerator for 5 min daily. Improvement was obvious after 2.5 months. After another 6 months with slightly over-correction, the appliances were removed and use refinement aligners to finalize the alignments and the outcome was satisfactory. No roots resorptions and other pathology were observed.
The CMA create a mesial out rotation around the palatal roots of the first molars and enhance the mandible to a forward position as the molars were de-rotating. Also, the lower were extruded due to upward vector pull from the elastics and therefore reduce overbites and promote changes on the occlusal plane. Stage I correct sagittal and stage II correct dental discrepancies. Rodriguez in 2019 reported the long-term sagittal stability of the treatment was good. (9) Popowich in 2005 reported for non-extraction Class II patients, the average times Class II elastic wear was about 10 months and 25.7 months for fix appliances. In the CMA sample, the first phase averaged 5.1 months (±2.8 months), and the second phase with fixed appliances was about 13.0 months (±4.2 months). The total treatment duration was 18.2 months (±4.8 months). Therefore, the advantages of CMA treatment were the reduced duration of elastic wear and overall treatment time. (8)
McNamara et al in 2012 traced 32 patients with serial of cephalograms at 3-time intervals: T1 (initial), T2 (removal of CMA), and T3 (post-treatment). The results were digitized, and superimpositions were constructed to compare the linear and angular variables with untreated subjects who were presented with normal facial profile and occlusions. Variable of ≥2.0 mm or ≥ 2.0°was used as an indication of clinical significance. They found the nature of treatment effects of CMA are dento-alveloar with only little skeletal changes. (4) These findings were also investigated by O'Brien and coworkers. They measured changes in skeletal and dentoalveolar changes used P value of <.05 to determine statistical significance instead of change of ≥2.0 mm or 2.0° of any cephalometric variables as indicators. However, the limitations of these kind of studies were retrospective nature and the use of historical controls. The mandible is brought forward by heavy elastics that were worn full-time by the patients during CMA treatment. The Co-Gn distance (mandibular length) increases during treatment when compared to normal growth. Nevertheless, there were no statistically significant in the increase of mandibular length. (4 O'Brien)
Hamilton in 2013 conducted a survey on 42 CMA patients and 70 patients treated with the fix appliances. The results suggested the CMA group feedbacks were more comfortable and more positive to the overall experience with less negative effects compared to the fix appliance group. In the adolescent patient, the CMA was shown to be more comfortable for the patient to wear, offered a more positive overall experience, and had fewer negative comfort-related side effects compared with other appliances for Class II treatment. (Hamilton) (5) There were no difference in the anteroposterior position of the chin at pogonion between the two groups. (2) Sandifer et al. in 2014 examined the treatment effects of the CMA using two mandibular anchorage protocols: a lingual arch and fixed appliances. There was successful correction of Class II occlusion immediately following the use of CMA, with minimal maxillary molar tipping observed during molar distalization.
Kim-Berman in 2019 found that the SNB angle decrease −0.8° in CMA patients. This decrease in the SNB angle could have been related to the increase in vertical skeletal relationships that occurred in the CMA sample with respect to the controls. There was no difference in anterograde-posterior position of the chin. He also found that the sagittal skeletal changes were similar for the CMA Class II group when compared to the fixed appliance group. There were possible restrictions of maxillary growth rather than mandibular advancement or enhanced growth. There were increased in mandibular plane angle and increase of Lower anterior face height observed. A clockwise rotation of the FOP relative to Frankfort was also reported. (2)
Thurzo in 2022 advocated to use personalized custom-made 3D printing device for the manufacturing of the distalizer. These hydbrid appliance designs are more aesthetic and increase patient compliance and co-operations. (10)
Summary of Changes Observed from CMA Treatment
Sagittal Changes in Maxilla:
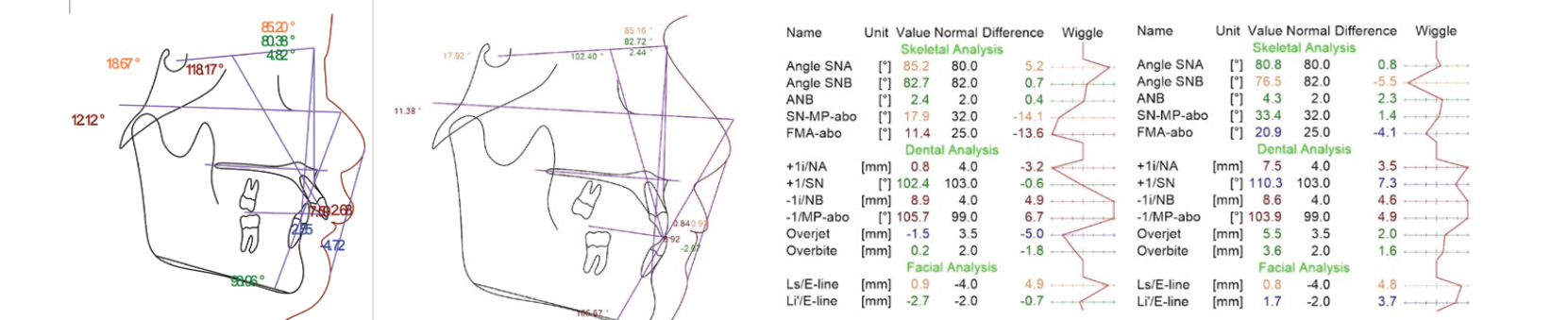
In both cases, there were no obvious SNA changes. In case 1, the distance from Point A to the nasal perpendicular was reduced by 2mm, and the distance from the Condylion to point A increased. The midfacial length increased in both cases.
Sagittal changes in Mandible:
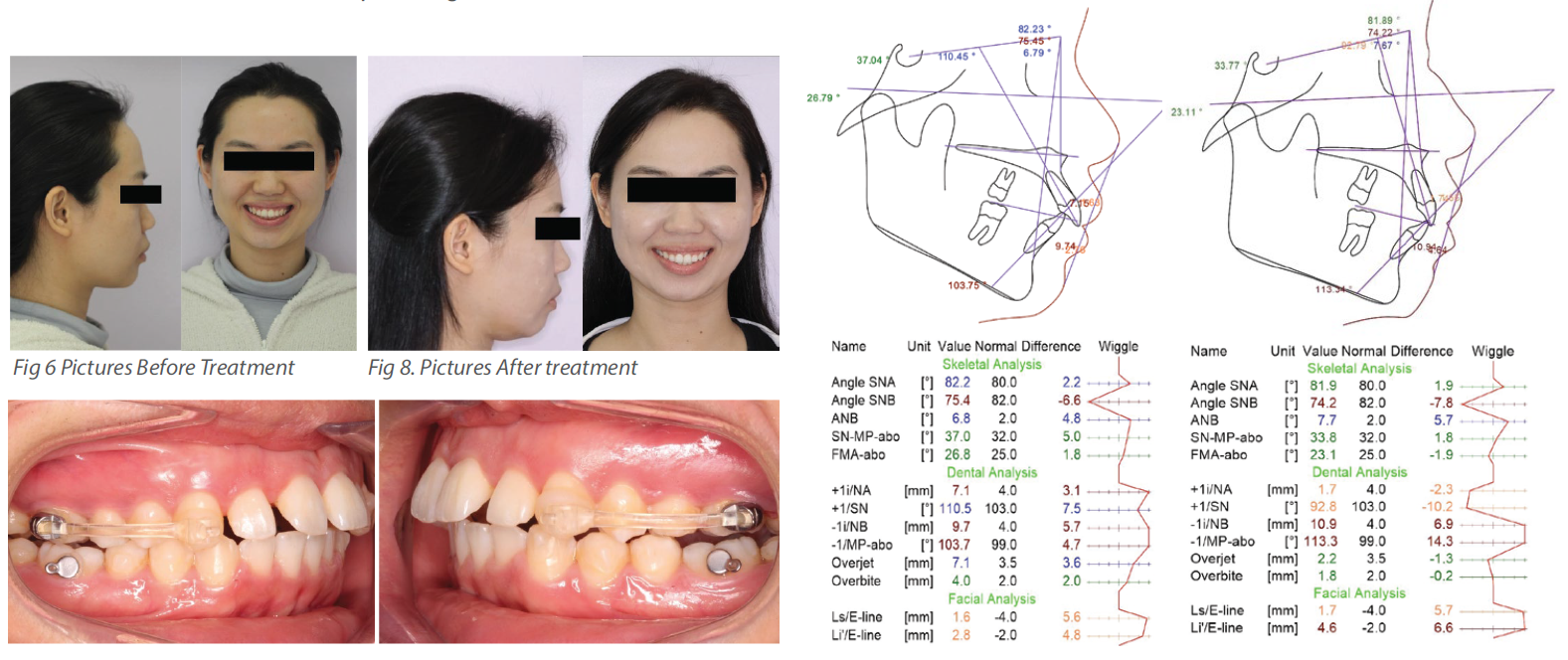
SNB increased slightly in case 1 but remained unchanged in case 2. The mandibular length Go - Gn increased 4 - 5 mm in case 1 and had zero increase in case 2 due to the patient's age and completed bone growth. The Pogonion moved anterior slightly.
Maxilla and Mandible Relationship:
The Wits appraisal values changed from 4 - 5mm to zero in both cases. There were slight changes of 1 - 2 degrees in the ANB values. The maxillo - mandibular differential, the difference between Co - Point A and Go - Gn, increased and moved toward a Class I relationship in both cases.
Vertical Skeletal Assessment:
In case 1, the anterior lower face height (ANS - Menton) increased without significant changes in the mandible plane angles. A clockwise rotation of the functional occlusal plane (FOP) relative to Frankfort horizontal was observed during phase I.
Dento - Alveolar Relationship:
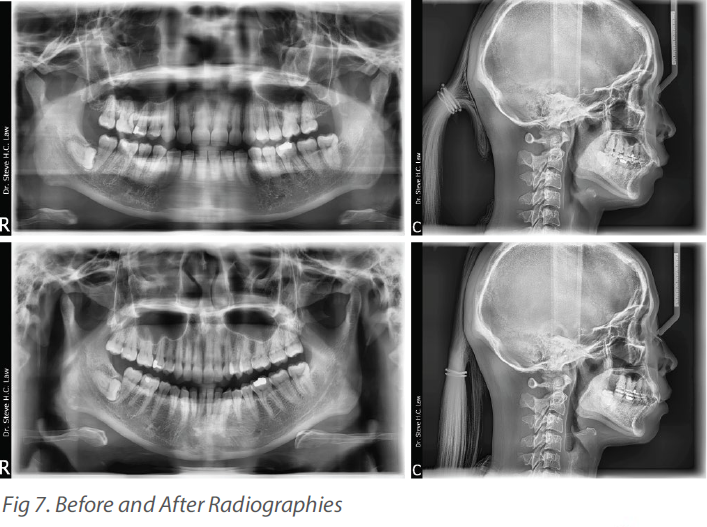
There were net molar improvements in both cases. The overjet improvements were obvious, from 10 to 0mm in case 1 and 8 to 2mm in case 2. The overbites changed from 90 to 10% in case 1 and 50 to 20% in case 2. Proclinations of lower incisors were also noted.
Skeletal Relationship:
There was a reduced forward movement of point A. The chin point at the Pognion remained in the same location. SNB decreased for both cases. The lower anterior facial height increased in case 1 (ANS to Menton).
Conclusions
The Carriere Motion 3D distalizer is efficient and effective for Class II malocclusion correction, causing less discomfort and increasing patient compliance and cooperation.
The effect is mainly dento - alveolar in nature, with changes in molar relationship, overbite, and overjet, combined with some lower incisor intrusion.
There are obvious skeletal changes and an increase in the lower anterior facial height.
Case selection is important since growing children with mandibular growth can benefit the treatment. It can be used for adults but provides better results for growing teenagers.
Mandibular length is not affected by treatment.
The pogonion chin point does not move forward due to the increase in the lower anterior facial height.